

Clonal mosaicism, detectable in peripheral blood, can be an important predictor of developing a hematological malignancy. We sought to determine if mosaic events, in addition to clinical and demographic variables, contributed independent information about acute lymphoblastic leukemia (ALL) patient survival and risk of relapse after allogeneic hematopoietic cell transplant (HCT).
HumanOmniExpress-12v1_A BeadChip SNP array data were used to detect mosaicisms >=2Mb based on the log2 relative probe intensity ratio (LRR) and B allele frequency (BAF) for each SNP measured in 773 ALL patients from DISCOVeRY-BMT cohorts. DNA was extracted from recipient peripheral blood samples taken immediately prior to start of conditioning before allogeneic HCT for ALL (2000-2011). Mosaic events include copy-number gain (LRR >0), loss (LRR <0), or copy-neutral loss of heterozygosity (CNLOH), defined as a deviation from BAF heterozygosity without LRR changes.
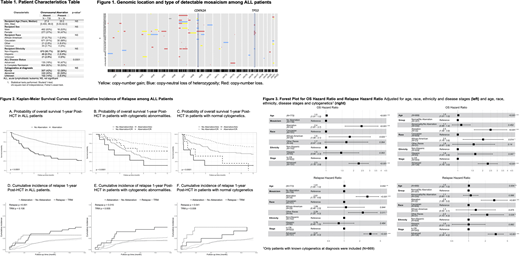
The impact of mosaicism on overall survival (OS) probability and cumulative incidence of relapse at 1-year post-HCT were calculated using the Kaplan-Meier estimator and cumulative incidence functions, respectively. The association of clonal mosaicism with OS was evaluated with multivariable Cox proportional hazard models. For disease relapse, competing risk models were used with transplant related mortality (TRM) treated as a competing event. Stratified survival analyses were performed by cytogenetic status at diagnosis. Statistical analyses were conducted using R 3.6.1.
Thirty-four patients (4.4%) had 1 or more mosaicisms (82 total detected) with almost half having advanced disease (Table 1). The median proportion of affected cells was 61% (interquartile range = 39 - 93%). Copy-number losses on chromosomes 7 (13.4%) and 9 (8.54%) and 17 (6.10%) were the most frequently detected events (Figure 1). OS at 1-year post HCT in patients with and without a mosaic event was 26.5% and 60.1%, respectively, (P=8.2×10-8, Figure 2A) and normal cytogenetic patients with mosaicism had significantly lower survival compared to all other patients (OSnormal/mosaic+= 8.3% vs. OS= 60.6%, P=3.0×10-10, Figure 2B-C). ALL patients with a mosaic event also had an increased risk of disease relapse overall (Relapsemosaic+= 50% vs. Relapsemosaic-=26%, P=0.00067) and when stratified by cytogenetic abnormalities (P=0.015) and normal cytogenetics (P=0.041) (Figure 2D-F).
Multivariable models of OS and relapse included age, race/ethnicity, complete remission or advanced disease status (Figure 3). Patients with a mosaic event had ~2.5 fold increase risk of death (P=2.5×10-5), independent from cytogenetics (P=8.6×10-5, Figure 3). OS associations are likely driven by the 2.8 fold increase risk of relapse (P= 5.9×10-5) which remains highly significant when stratified by cytogenetics (Figure 3).
Almost half of the copy-number losses included well-known regions on chromosomes 7, 9 and 17 (Figure 1). Deletions of 7p have been shown to correlate with lower event-free survival in ALL pediatric patients. Our findings suggest mosaic loss of 7p might be an important indicator of poor OS across the lifespan, with 5/6 patients with 7p losses aged >18 years. Higher mortality was also associated with the loss of the chr9p21.3 locus, seen in all patients (N=5) with chromosome 9p losses. This region harbors tumor suppressor CDKN2A; inactivation of CDKN2A can lead to poor survival in both children and adults with ALL. Lastly, we found that all patients (N=4) with copy-number loss of 17p13.1, which contains tumor suppressor TP53 died within 1-year post-HCT.
We identified detectable mosaicism prior to transplant in 4.4% of patients and showed that mosaicism was associated with lower survival and higher disease relapse at 1-year post-HCT. While mosaicism is more common in patients with advanced disease stage, mosaic events are an independent contributor to lower survival and higher relapse in the first year after transplant. This is the first study to show that mosaic events detectable in pre-transplant peripheral blood from ALL patients are correlated with poor survival. Future studies replicating these associations in different ethnicities and age groups and evaluating specific chromosomal regions could be informative in classifying patient risk post-HCT attributable to mosaic events.
McCarthy:Karyopharm: Consultancy, Honoraria; Magenta: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Advisory Board; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Advisory Board; Takeda: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Advisory Board; AbbVie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Advisory Board; Genentech: Consultancy, Honoraria; Starton: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Advisory Board; Juno Therapeutics, a Bristol-Myers Squibb Company: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Advisory Board , Research Funding is to Roswell Park, Research Funding. Pasquini:Bristol Myers Squibb: Consultancy; BMS: Membership on an entity's Board of Directors or advisory committees, Research Funding; Amgen: Other; Novartis: Research Funding; Kite: Research Funding. Lee:Pfizer: Consultancy, Research Funding; Novartis: Research Funding; Takeda: Research Funding; Amgen: Research Funding; Kadmon: Research Funding; Incyte: Consultancy, Research Funding; AstraZeneca: Research Funding; Syndax: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal